 From 30 to 75%: Range of motion milestones – Keeping my head up high
From 30 to 75%: Range of motion milestones – Keeping my head up highWarning: The NCBI website requires JavaScript to operate. Functional anatomy of cervical spine and biomechanics of lesions due to compressed loadErik E Swartz*New Hampshire University, Durham, NHR. T Floyd†University of West Alabama, Livingston, ALMike Cendoma‡Sports Medicine Concepts, Inc, Geneseo, NYErik E. Swartz, PhD, ATC; R. T. Floyd, EdD, ATC; and Mike Cendoma, MS, ATC, contributed to design and writing, critical review, and final adoption of the article. AbstractObjective: Provide a knowledge base on functional anatomy, kinematic response and mechanisms involved in the lesion of the axial-compression cervical spine in relation to the sports injury. Data sources: We perform literature searches through the databases Index Medicus, SPORT Discus and PubMed and the Library of Congress from 1975 to 2003 using the key phrases cervical spine lesions, cervical spine biomechanics, spinal football lesions, cervical spine kinematics and axial load. Data Synthesis: Research on normal mechanisms of kinematics and minor and greater lesions to the cervical spine reveals the complex nature of the movement in this segment. The movement in a single plane is not the product of the equal and summary movement between all cervical vertebrae and between them. Instead, individual vertebrae can experience an investment of movement while traveling through a single plane of movement. In addition, the vertebral movement in 1 plane often requires movement contributed in 1 or 2 other planes. Injury mechanisms are even more complex. The reaction of the cervical spine to an axial-load impact has been investigated using specimens of corpses and demonstrates a pandemic effect. The location of the impact and orientation of the head affect the resulting degree and level of injury. Conclusions/Recommendations: As with any joint of the body, our understanding of the mechanisms of the cervical spinal injury will ultimately serve to reduce its occurrence and increase the likelihood of recognition and immediate attention. However, the cervical spine is unique in its normal kinematics compared to the joints of the extremities. The biomechanics of lesions in the cervical spine is complex, and you can still learn a lot about the mechanisms of the cervical spine injury specific to sports. Due to the potentially catastrophic nature and disruption of the life of the cervical spine lesion (CSI), there is a lot of concern regarding the prehospital management of the injured athlete of the cervical spine. This is evidenced by a multi-professional effort of the working group initiated by the National Association of Athletic Trainers to establish general guidelines for the acute care of the athlete injured by the spine. The main ISCs, although rare in comparison to the lesions of sprain and strain to the extremities, are worrying due to mortality rates and the possible permanent loss of neuronal function. A CSI requires an immediate and deliberate but sensitive response. The highest rate of serious neck injuries has occurred in football and rugby. Other sports and activities that contribute to a high rate of CSI are fighting, diving, recreational diving, ice hockey, gymnastics and horse riding. The most severe CSIs associated with athleticism can be attributed to axial loading compressive forces. Clinically, an important CSI results in the committed integrity of the cervical segment due to fracture, dislocation, subluxation or ligamentous tear, leaving the cervical spine unstable. White et al defined clinical instability in the spine as more than a horizontal displacement of 3.5 mm from one cervical segment in another. Obviously, the athletic coach cannot detect the presence of such a tiny irregularity in the structure of the spine and must therefore assume the worst scenario. Motion in a plane in the cervical spine requires the contribution of the complementary movement of individual vertebrae in other planes. This further complicates the kinematics of the cervical segment and the resulting injury mechanisms. Considering the injury mechanism is an important first step in evaluating any athletic lesion in the field. An athlete with a significant spinal cord injury may not present immediately with emerging signs and symptoms. Therefore, the understanding of cervical spine kinematics is important for the athletic trainer, not only to help appreciate the following sections regarding injury mechanisms, but also to allow a more effective evaluation tool after CSI. The purpose of this literary review is to provide a knowledge base on functional anatomy, the kinematic response and the primary mechanisms involved in the CSI during the participation in sports, specifically regarding axial-compression forces. A secondary purpose of this review is to demonstrate the need to investigate the mechanisms of sports injuries of the cervical spine. ANATOMY FUNCTIONAL The range of movement of the cervical spine is approximately 80° to 90° bending, 70° extension, 20° to 45° lateral bending and up to 90° rotation on both sides. However, the movement in the cervical spine is complex, because the pure uniplanar movement does not accurately portray the movement between the cervical levels, and the movement in any range is not the simple sum of equal movement of a vertebra to the next. Normal spine kinematics The first cervical vertebrae, the atlas, has often been labeled the cradle, because its joint with the occiputum of the skull provides a cradle to support the head (). The atlas articulates with the occipital condiles, and their primary movements are bending and extension. Normal bending to hyperextension in atlanto-occipital joints varies from approximately 15° to 20°. The rotation and lateral bending between the west and the atlas are not possible due to the depth of the atlantal basins, where the occipital condiles rest. Rotation on the one side makes the occipital condyle contralateral contact the previous wall of its atlantal intake and the ipsilateral condyle to contact the back wall of its respective intake atlantal. Similarly, lateral bending requires that the counter-lateral occipital condyllium emerge from its take, a movement that is restricted by the tight atlanto-occipital joint capsule. The weight of the head is transferred to the cervical spine through the atlanto-axial side joints of C2, the axis (see ). The odontoid process that extends from your body rests within a facet in the atlas that is created by the previous arch and allows the atlas and head to turn side by side as a unit. The normal rotation ranges of C1 in C2 are 50° each side. However, the results have varied, and it has been observed that this range is 32° in corpses, of 75.2° through radiographic techniques and 43° by computed tomography. However, this rotational capacity of the atlanto-axial joint is possible due to the stabilizing function of 3 primary ligaments (transverse, alar and apicales), which act to keep dens as a "fixed bet" in which the atlas can rotate. Rotation is also possible in C1 to C2 because, unlike the atlanto-occipital articulation, the upper and lower side joint facets of the atlas and axis create a biconcave surface. The concavity of each joint surface is due to the articular cartilage of the lower and upper facets and is not visible on a radiograph. This feature allows the previous and later translation of the joint surfaces, and as the atlas continues to rotate, it sits on the axis as the upper joint process on each side slides down the previous and later edges of the lower convex surfaces. The biconvex nature of the atlanto-axial joint means that the bending and extension of the cervical spin often create movement in the opposite direction that is experienced in the atlas. Thus, when the cervical spine bends, the atlas spreads, and when the cervical spine spreads, the atlas flexes. This coupling movement is possible because the atlas is balanced in the concavity of the axis, and when the compression line moves prior to this point of balance, as when the neck extends, the atlas moves in bending. The reverse follows as the reflections of the cervical spine, moving the compression line after the balance point and creating extension in the atlas. This coupling, or movement investment, is a unique feature of the spine, can be experienced at different levels, and will also be important in understanding the injury mechanisms ().A, Translation. B, Extension of C1 creating flexion in C2. C, C1 Flexion creating extension in C2Another characteristic of the atlanto-axial joint also found in other segments of the cervical region is that the pure rotation of the atlas in the axis does not occur without a small degree of lateral extension and bending and sometimes flexion. Once again, the line of vertical forces that are distributed across the west to the atlas while the head moves determines the amount of movement of coupling in the atlas, as it balances between the head and the axis. Normal cervical spine kinematics In the C2 to C3, the upper cervical spine is found with the remaining, most typical cervical spine. The axis body acts as a "raice" within C3, ensuring the upper cervical spine in the remaining cervical spine. The articulating surfaces of the lower and upper intervertebral joints are similar to a sillin joint, maintaining pre-posteral and median concavities and laterally directed. This orientation of the cervical bodies in the middle to lower cervical column allows rotation and bending movements but is resistant to lateral bending. Side bending is possible as a combined movement in the cervical spine, but only because of the rotational movement united in each segment on that side. The general bending and neck extension movement does not necessarily reflect the movement between vertebrae in the cervical spine. In fact, a vertebrae may experience its largest range of motion or extension inflection before the cervical spine itself has fully flexed or extended. In addition, a vertebrae may experience a wide variety of motion in an address while the cervical spine throughout the exposure moves in the opposite direction. The order of contribution of the cervical segments to the bending and extension also varies by level. Through high-speed filmradiography, Van Mameren et at the time determined that the bending begins in the lower cervical column (C4 to C7), followed by the C0 (occust) movement through C2, C2 to C3, and then C3 through C4. The C6 to C7 segment experiences a brief investment of the extension motion, followed by an investment of the C0 motion through C2. The C6 to C7 segment contributes to the final ranges of bending. The extension also starts in the lower cervical spine (C4 to C7) and is followed by the beginning of the C0 movement through C2. The average range consists of a varied movement from the middle cervical region, while the lower cervical column is the last to contribute as the column moves towards the terminal extension. This unique movement characteristic of cervical vertebrae is explained by Penning and Amevo et al through a concept known as the instant rotation center (ICR). The rotation center for a particular vertebrae is actually close to the upper aspect of the lower vertebral body () and can be used to explain the movement investment observed in the cervical spine. The "reversion of the curve" that occurs in a vertebrae is due to its role as a pivot point in the cervical spine. As the force lines are passed through the cervical spine, the vertebrae experience bending or extension depending on the location of the force vector relative to the ICR. Therefore, if the cervical spine moves in bending, but the force vector passes behind the ICR of a specific vertebrae, then that vertebrae will spread. Penning used the ICR theory to describe the biomechanical lesion in the cervical spine. The reversal curve phenomenon in the cervical spine segment is further clarified through the work of Nightingale et al in the analysis of lesions to the cervical spine during the "coup" and discussed later. INJURY BIOMECHANICSIn the early literature of CSI, researchers focused on the movement of the head during the injury and attributed the primary mechanism of suspected lesion in the cervical spine to that specific movement. However, a more recent study has shown that the motion observed in the head during the injury is not a reliable indicator of the spinal movement responsible for creating the injury. Biomechanics in the spine and the degree of spinal injury depend on the location of the impact on the head and the orientation of the cervical spine at the time of impact. The initial injury, and often the most critical, occurs as soon as 2 to 30 milliseconds after impact, well before the movement in the cervical spine and the head occurs. Axial Charge in Football The injury mechanism that has received the greatest attention in athletics is the axial load. Only 13 per cent of the 209 football-related injuries that resulted in the permanent cervical quadruple between 1971 and 1975 were due to hyperflexion (10 per cent) and hyperextension (3 per cent), while 52 per cent were attributed to the axial load. According to the National Center for Research on Catastrophic Deporative Injuries, a total of 107 cases of permanent cord injury in football were produced between 1977 and 1989, with the most important results of manipulation. More recently, 15 cases of quadrilateral were reported in high school football between 1991 and 1993, with the main cause attributed to the axial compressive burden. The axial load occurs when the head and neck are flexed to approximately 30°, as in a foreground. In this position, the normal manor curve disappears, which eliminates the elastic energy absorbing component of the region. When the contact applies to the head crown or helmet on the football player, the cervical spine experiences a compressive load of the torso. As the filler provided by the helmet reaches its absorptive limits, the head reverses the direction, resulting in an increased compressive load as the cervical spine is compressed between the head and the torso. When this compressive force exceeds the absorption capabilities of the column, the components of soft and hard tissue fail. The compressive load limits of cervical vertebrae are estimated at 3340 to 4450 N. Curiously, the upper compressive load limits of the cervical spine have been reached in less than 11 milliseconds during simulated impacts using a speed and mass equivalent to about half of those of a conditioned athlete. Furthermore, CSI occurs when the compressive loads in the cervical spine are increasing at a growing rate, demonstrating that during an axial load, the potential for serious neck injury exists independent of the neck force. Too often, these lesions are caused by a conscious effort to launch, or use the head crown as an initial contact point during an approach. Despite the changes in the rule, team improvements and a general decrease in the number of catastrophic lesions resulting from these significant epidemiological findings, the appearance seems to be as prevalent now as before. Cervical Spine BucklingDuring the axial load in the cervical spine, the compressive forces result in a transient deformation or thinning effect. This pandeo produces large angulation within the cervical spine as a means of releasing the additional strain energy that has occurred from the vertical load and is the causative factor of the lesion (). Nightingale et as they evaluated the dynamic responses of the cervical spine to the axial load through high-speed videos and specimens of eachver mounted (inverted) to a drop-down device. The stalking occurred in 1 of 2 separate orders. The first-order elongation resulted in the extension of the upper cervical column through C5 and the bending through T1. The bending of double order created C1 to C3, extension in C4 and C5, and bending in C6 to T1. The levels in which the column reverses its movement are where pivot points have been created, as in the abrupt curve investment described above. Hebillas and lesions occurred in specimens within 2 to 31 milliseconds after impact, well before an observable movement was observed in the complex head and neck (20 to 100 milliseconds). In essence, a cervical vertebrae can almost immediately be placed in an extreme position of hyperflection or hyperextension during the pandemic, although the head and neck complex is not yet experiencing observable movement. This fact is critical for the athletic trainer to understand: the movement in the head is not a reliable indicator of motion at various levels of the column; therefore, the injury potential should not be underestimated. Although the investigation of human injury mechanisms with the bodies is valuable, a limitation lies in the inability to explain the contribution of the forces and the joint stability of soft tissues. Although the injury occurs before the approximate time of reflexive muscle contraction (60 milliseconds), it may be assumed that there is some degree of muscle activity and stiffness in the athlete's cervical spine at the time of impact. In addition, to our knowledge, most of the research carried out on vertical biomechanics and axial loads have involved loads applied to a specimen of cadaver in vertical direction. Few cases in sport place the athlete in a pure and inverted position when receiving an axial load. More often, the player intentionally decreases the head or fall, and the head and trunk travel in a parallel or oblique direction relative to the ground. The effect of gravity, along with the static stabilization of the subsequent muscles at the top of the back and the cervical region in these situations, could affect the balance mode and the direction of the resulting force vectors. The researchers have not so far attempted to simulate these internal and external forces in a non-vertical position and their effect on the imminent injury, and have not assessed the effect of adding mass and size to the head, as when they wear a helmet. More research is needed in this area specific to the functional demands and mechanisms of sports injury. Head orientation and padded surfacesNightingale et evaluated the dynamic response on the corpses to the axial impacts by adjusting the contact-surface orientation so that the head was impacted prior to the vertex of the head (15° and 30°), on the vertex (0° or midpoint), or after the vertex of the head (15°). The greatest degree of injury was when the impact was on the vertex or prior to the vertex of the head, without lesions in the cervical spine with a post-verthice impact. For the previous impact conditions and vertex, only 2 out of 6 specimens did not experience injury, while 2 specimens experienced multiple-level injuries. The authors correlate the risk of injuries to the impact location. Specifically, when the head experienced a direct or prior impact on the vertex of the head, the neck load vector responsible for moving the head off the torso road was too small and could not speed the head off the road before the injury occurred. However, the more the impact point is in the back direction, the easier it is for the cervical spine to bend and move the head out of the torso's main force path. Nightingale et al also investigated the impact on padded surfaces. The padded surfaces within the helmets are used worldwide in sport and act as protective coverage for the extremities and objects such as goal poles. However, the relationship of this padding has not been established with the kinematics of the cervical spine. Researchers, in fact, have not shown that filling acts to protect the cervical spine, and have even been shown to increase the likelihood of lesion greater than the cervical spine. Using the same methods of drilling and orientation of the impact platform, researchers covered the rigid surface with a padded material. Impact forces on the head decreased, as expected, but the resulting neck forces increased, causing more serious injuries than with unpaid impacts, regardless of impact orientation. The greatest impulse, due to the padding, allows the impact forces to be experienced in a longer time, and in most scenarios in sport, this is desirable. However, with respect to the cervical spine, the longer the head is placed in axial compression, the longer the harmful forces are applied to the neck. Therefore, the filling creates a "pocket" for the head during the impact. This pocket makes the head depress on the surface of padded foam, which acts to "put" to the head. Therefore, a pocket event increases the risk of lesion to the cervical spine due to increased time of exposure to compressive force. The effects on the head in contact sports are often found on a surface with a certain degree of filling. This may include filling on the equipment, a pad used by an opponent, a soft tissue of an opponent, compressive playing surfaces, or stuffing inside the helmet itself. All these situations may present some degree of bottling, which makes it much harder for the spine to escape from an axial load. Although the presence of filling provides a risk to the CSI, its use is necessary to protect against the most commonly present blunt trauma in the sport involving the skull or other anatomical structures. Athletic instructors should consider the type of impact surface involved in a CSI suspect and, according to the findings of the investigation, they should appreciate the potential severity of the injuries due to pocket placement and impact orientation. Whiplash Although it is more common in automotive accidents, the injury of the blender can also take place in contact sports. An example of a batting type injury in football occurs when the quarterback is fired from behind, especially if the quarterback does not expect to be beaten. However, contrary to what is generally considered as an injury caused by an extreme range of movement in the head or neck, some cervical injuries from the smoothie are due to compressive forces. The difference in the mechanism between the splash and the typical axial load is that the compressive force is directed superiorly from the cervical spine, rather than a force directed less than the axial load. The combined efforts of several researchers using human subjects, cadaver specimens and mathematical modeling have provided a detailed time of events in the cervical spine during the smoothing to explain the sympathetic mechanism. The first joints and segments of the body to experience the movement during a smoothie are the hips, back and trunk. These body structures not only progress after a rear collision but also upwards. This ascending thrust of the trunk compresses the cervical spine. Along with the forward movement of the trunk, this combination of movements makes the head turn backwards in the extension, creating tension and balance where the lower cervical segment and the upper cervical segment flexes are spread. The neck peak extension during the blender is 45°, which is not beyond the normal physiological limits of the neck and therefore is not the real cause of injury. Rather, the harmful mechanisms (compression, forward displacement of trunks, and pandeo) act together to abnormally rotate individual vertebrae in extension. As a vertebra experiences this rotation, the previous components are separated and the subsequent components, in particular the facet joints, experience extreme compression. The minor fractures of the lower joints of the facet have been discovered in specimens of corpses and during the autopsy on corpses after the vehicle crashes. Therefore, the lesion in the vertebral region is not necessarily due to hyperextension of the cervical spine excessive. Rather, an individual vertebrae placed between the flexed and extended regions of a pandemic column extends around an abnormally high rotation axis, which forces it to the upper facet joints of the underlying vertebra (). By describing the events that occur during the smoothie, most researchers have studied topics sitting in car seats with headrests. However, the type of batting injury in the sport, in addition to competitive car racing, is more likely to occur when the athlete is in a vertical position without a head restriction. The upward thrust of the torso may not be as large in a vertical position as in a sitting position, possibly minimizing the pande and compression effect. However, abnormal rotations can still occur in vertebrae, especially because there is no post-head and neck restriction. If the initial radiographs do not reveal cervical fractures after the sieve, the diagnosis is usually generalized to the injury of the soft tissue, and no further diagnostic techniques are pursued. However, threats to the integrity of the cervical columns remain possible from the symbolic and cannot be clearly identified with any radiographic technique, which can result in an underestimation of the recovery time. The investigation of the real mechanisms and injuries resulting from the specific silencing of sport is justified. Pressure lesionsThe spine injury and permanent string damage can occur even if the soft and bear tissues remain intact. Imagine the hard sack like a water-filled balloon. As the balloon is bent or tightened in the middle section, the balloon diameter at the squeezing site decreases as the water inside the balloon flows away from the increased pressure site. As water accumulates on both sides of the restricted area, the ball is destined as the volume of water increases, greater stress is applied to the walls of the globe. Normal movements of the cervix apply standard pressure changes to the spinal cord that do not result in injury. However, when the neck is subjected to extreme ranges of motion at high speeds or in the presence of cervical canal stenosis, excessive pressure can be applied to neuronal tissues. If this stress exceeds the resilience of the neuronal tissue, these structures can be compromised, as well as the excessive or rapid extremism of a water balloon can cause the balloon to break. The pressure experienced by the marrow and changes in the geometry of the spinal canal under axial load have been investigated by Chang et al. Specifically, these researchers measured diameter changes in the spinal canal and the height of the segment of the cervical spine during the axial induced lesion in 10 specimens of the cadaver. The authors prepared the cervical spine segments of the body with the spinal cord removed and placed a water-borne tube in the spinal canal to measure the occlusion created during the impact. Then a weight of 5.95 kg was vertically reduced from a height of 1,53 m. In 8 out of 10 specimens, the tube in the spinal canal was completely ocluded at the time of the injury. In addition, specimens experienced an average decrease in the height of the spinal segment of 8.9 mm at the impact point, only to recover 35% of its original height. Clearly, at the time of the axial-load impact, the cervical spine and the spinal canal experience important transient geometric changes. Spinal cord injuries are often described as marrow bruises and are probably a direct result of the decrease in the diameter of the canal. After this injury, the neuronal tissue responds like any tissue in the body to a concussive force, which can result in neurapraxia or spinal shock. Therefore, the bone marrow injury may be present even with negative radiological findings and a stable spinal segment. Careful and detailed neurological evaluation should be performed after spinal shock to ensure the complete resolution of the initial inflammatory phase. CONCLUSIONSAs is the case of each joint of the body, our understanding of CSI mechanisms will ultimately serve to reduce its occurrence and increase the probability of immediate recognition and proper care. However, the cervical spine is unique in its normal kinematics. The biomechanics of lesions in the cervical spine is complex, and you can still learn a lot by continuing research on the reaction of the cervical spine to the specific injury mechanisms for sports. In addition, athletes who are placed in positions known to be associated with spinal cord injury are at increased risk of injury and paralysis in the spinal cord. Athletic instructors should not only understand the injury mechanisms to the point of being able to recognize them in the field, but also be able to prove that it is often the decision of an athlete to place themselves in a compromised position leading to the injury. REFERENCESFormats: Share , 8600 Rockville Pike, Bethesda MD, 20894 USA
What is neck flexibility? More Exercises to Improve Your Range of MotionThe black bending is the action to move your chin to your chest. Although it is a simple movement, it is possible to develop pain, and reduced mobility in this area. The causes may include actions as simple as looking down on your phone repeatedly, keeping your head in a position, or sleeping incorrectly. Read more about neck bending along with exercises you can do to develop strength, improve posture and increase your range of motion. The bending of the neck is the movement to lower the chin to the chest. This occurs in the joint just below the skull and uses deep neck flexor muscles, as well as . Others include: In the bending of the neck, a normal range of motion is 40 to 80 degrees, which is measured by a device called goniometer. This shows how far you can move your neck without experiencing pain, discomfort or resistance. Healthy joints, muscles and bones help maintain a normal range of motion. The bending of the neck with disabilities or limited has a variety of causes and usually involves actions that require you to look often. When it is the result of looking down on a portable device, it is known as . Activities that can cause stiffness in the neck and include: The following exercises build strength, relieve pain and increase the range of movement in the neck and upper back. You can do these exercises while sitting or standing. Use slow and controlled movements and avoid forcing any movement. When moving your neck, keep the rest of your body still to keep the correct alignment and posture. The bending stretch in the neck This exercise will help loosen your and reduce stiffness. To deepen this, put a hand behind your head with your fingertips at the base of your skull to help guide the movement. Neck Retraction This exercise loosens tight muscles, relieves pain and reduces spinal pressure. Keep your eyes ahead all the time. The aim of these exercises is to decrease the intensity and severity of the symptoms. These stretches relieve tension and pain in the neck, making them the perfect counterbalance for activities that require you to look repeatedly. Extensions of neck up This exercise points to the front of your neck. You can do this exercise by moving with each breath instead of keeping the position. Inhale while you look up and exhale while you return to the start position. Hang the bed Do this exercise when you wake up or before bed to relieve pain and increase circulation. This exercise allows you to turn your neck further, which makes it easy to check traffic when driving and spin quickly when playing sports. Neck Rotation You will feel this stretch along the side of your neck. Apply soft pressure to your chin to deepen rotation. These exercises help stretch shoulders and sides of the neck. To deepen this, use your hand to apply soft pressure to your head. If comfortable, stretch the SCM muscle by gently lifting the chin while in the stretch. Escalene Extreme This exercise works the lateral neck muscles that connect to your ribs. Although it is normal for neck concerns to develop, there are many things you can do to prevent or help them. Improve your posture The easiest way is to work on improving your and avoiding the stalking or letting your head go ahead. Make a habit of checking with your posture at all times throughout the day. Do not feel for long periods of time If you have to sit for long periods, get up and move for at least 5 minutes each hour. Do some or a little hike during this time. Keep your computer screen eye level Use a tray or table to change to your computer or workspace if you are doing something that requires you to search for long periods. Adjust your sleep position To maintain a neutral head position, . Avoid sleeping in the stomach. Use a pillow that allows your head and neck to rest in a straight position. Other recommendations See a doctor if you have recurrent injuries, pain that gets worse when you do these exercises, or severe pain that doesn't go away. You should also talk to a doctor if you have pain during normal activities, your symptoms are removed from the center of your neck, or your pain is accompanied by numbness, tingling or weakness. Neck bending exercises can provide quick relief for neck pain and stiffness, help build muscle strength and restore mobility. Do these exercises in short sessions all day, as part of a longer fitness routine, or to warm up or cool. Find what moves are helping or making your progress difficult and adjust if you need. To prevent recurrent pain, keep stretching daily even after you start to feel better. Last medical review on September 9, 2019Read this following

Neck Assessment | Musculoskeletal Key | Download Table")
Maximum Active Neck Range of Motion (degrees) | Download Table
Neck Assessment | Musculoskeletal Key
Facebook
Normal cervical spine range of motion using digital inclinometer in male asymptomatic subjects of Aseer, Saudi Arabia Alahmari KA - Saudi J Sports Med
prehab-exercises-amass-method-basic-assessments-for-running-cervical-spine- range-of-motion-head-and-neck-mobility - Prehab Exercises
The assessment of the cervical spine. Part 1: Range of motion and proprioception - Journal of Bodywork and Movement Therapies
Normal Range of Motion - Order
Cervical range of motion in lateral flexion and rotation, Muscle... | Download Table
Normal cervical spine range of motion using digital inclinometer in male asymptomatic subjects of Aseer, Saudi Arabia Alahmari KA - Saudi J Sports Med
Don't neglect your neck during training | Toronto.com
To What Degree Does Active Cervical Range of Motion Differ Between Patients With Neck Pain, Patients With Whiplash, and Those Without Neck Pain? A Systematic Review and Meta-Analysis - Archives of Physical
Top 5 Exercises for Increasing Range of Motion in Your Neck | The Blog of Dr. Nicholas Carlisle - Atlanta Chiropractor
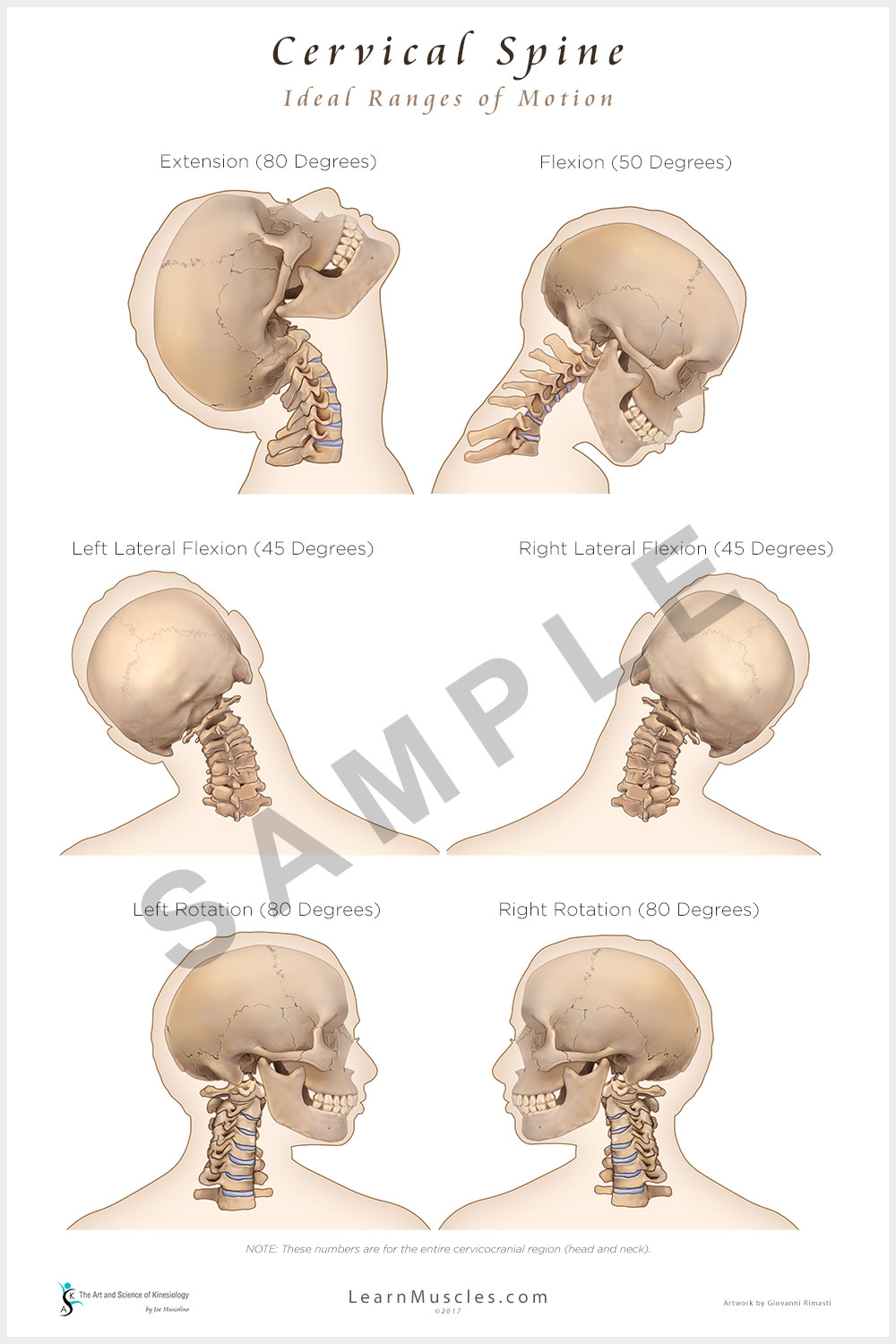
Pin on Shoulder Examination![Cervical Spine - Ideal Ranges of Motion 24]()
Cervical Spine - Ideal Ranges of Motion 24" x 36" Premium Poster - Learn Muscles
How to alleviate neck pain | KX Yorkville
How can owls turn their head for all 360 degrees? - Quora
Why EMS Should Limit the Use of Rigid Cervical Collars - JEMS
Axial and nonaxial ranges of motion of the Cervical Spine
Neck Assessment | Musculoskeletal Key | Download Table")
Maximum Active Neck Range of Motion (degrees) | Download Table
Restoring Your Body's Function After An Injury - prohealthcareproducts.com
Range of Motion
Sensors | Free Full-Text | An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors | HTML
NECK EXERCISES - ACTIVE CARE PHYSIOTHERAPY CLINIC")
Motion is Life- Especially in the Cervical Spine (Neck Pain Support Blog)
Increasing Your VA Rating for Back Pain and Back Injuries
Agreement and reliability of two non-invasive methods for assessing cervical range of motion among young adults
Topical Menthol Gel versus a Placebo Gel on Post-manipulation Pain and Range of Motion in Patients with Mechanical Neck Pain - PT Aligned | MeyerPT Physical Therapy Supplies
At Home Self Exam Neck Exam- Range of Motion Secrets
Figure 1 from Neck range of motion measurements using a new three-dimensional motion analysis system: validity and repeatability | Semantic Scholar
neck range of motion exercises | Family Health Chiropractic
PROCEDURE FOR NECK AND TRUNK RANGE OF MOTION :- SAMARPAN PHYSIOTHERAPY CLINIC AHMEDABAD
Baseline - fab-12-1076 Large Joint Arthrodial Protractor Goniometer to Measure Joint Limits, Range Of Motion, Cervical Rotation, Lateral Flexion and Anterior-Posterior Cervical Flexion in Active / Passive Movement: Construction Protractors: Amazon.com ...
Health&Fitness101 - Alpine Physical Therapy
Types of Body Movements | Anatomy and Physiology I
At Home Self Exam Neck Exam- Range of Motion Secrets
Dry Needling Can Instantly Improve Your Neck Range of Motion! - Specialized Orthopedic Physical Therapy
Proper neck warm ups
Cervical collars – why do they help some people and not others? – Caring Medical Florida





{kind=link}
Posting Komentar untuk "neck range of motion"